 Evolution
Evolution
 Intelligent Design
Intelligent Design
 Medicine
Medicine
Vasoconstriction and Platelet Aggregation Defy Evolutionary Explanations
Editor’s note: Physicians have a special place among the thinkers who have elaborated the argument for intelligent design. Perhaps that’s because, more than evolutionary biologists, they are familiar with the challenges of maintaining a functioning complex system, the human body. With that in mind, Evolution News & Views is delighted to present this series, “The Designed Body.” For the complete series, see here. Dr. Glicksman practices palliative medicine for a hospice organization.
 To feed the cells of the body so they will live, grow, and work properly, the heart must pump blood with enough pressure through the circulatory system. However, just as water under pressure can leak out of a pipe that has burst, so too a ruptured blood vessel can result in blood loss. Moreover, depending on how much blood is lost and where it takes place in the body, this can lead to significant health risks. Our earliest ancestors needed to live active lives and, just like us, were constantly at risk of blood loss from injury. If the body didn’t have the wherewithal to prevent significant blood loss, humanity could never have survived or reproduced.
To feed the cells of the body so they will live, grow, and work properly, the heart must pump blood with enough pressure through the circulatory system. However, just as water under pressure can leak out of a pipe that has burst, so too a ruptured blood vessel can result in blood loss. Moreover, depending on how much blood is lost and where it takes place in the body, this can lead to significant health risks. Our earliest ancestors needed to live active lives and, just like us, were constantly at risk of blood loss from injury. If the body didn’t have the wherewithal to prevent significant blood loss, humanity could never have survived or reproduced.
As I noted in my last article, the process that performs the important task of preventing blood loss is called hemostasis. Hemostasis involves the quick and almost simultaneous actions of the injured blood vessel, the platelets, and the clotting factors to form a fibrin clot to stop the bleeding.
But the body faces another dilemma. A clot in a major vessel like an artery supplying blood to the brain, or the heart, or the lungs, can cause significant damage. In other words, hemostasis and the clots it forms must turn on only when it’s actually needed and must turn off and stay off when it’s not. It’s like the sprinkler system in a factory and an air bag in a car. They must deploy only when needed. Let’s consider the first two components of hemostasis: blood vessel vasoconstriction and platelet aggregation.
Just like in a garden hose, there is a central channel or lumen through which blood flows in a blood vessel. The tissue that lines the lumen is called the endothelium. The endothelium does much more than just act as a barrier between the blood and the underlying support tissue, which in most blood vessels contains a protein called collagen and is surrounded by muscle. When a blood vessel is injured, local chemical changes related to the endothelium trigger the surrounding muscle to automatically contract in an attempt to close down the lumen to prevent further blood loss.
This short-lived vasoconstriction plays a major role in hemostasis and often in small arteries and arterioles can almost totally shut off the blood vessel, allowing the platelets and clotting factors to work together, forming a clot to permanently seal the injured site. Vasoconstriction acts like the person who has to sit on an over-packed suitcase so the top and bottom can be brought close enough together for the lock (platelet plug and fibrin clot) to be applied. Without vasoconstriction, the task of the platelets and clotting factors would be impossible.
Adequate hemostasis to prevent recurrent serious bleeding would have required our earliest ancestors to have blood vessels with normal function. There are several rare medical conditions in which the body has abnormal blood vessels that have difficulty contracting upon injury. Some chronic illnesses cause significant vascular fragility. These conditions put people at very high risk for bleeding from minimal trauma, resulting in life-threatening hemorrhage if a major organ or blood vessel is involved.
Evolutionary biologists may imagine how blood vessels came into being, but clinical experience shows that the complicated structure of blood vessels must not only allow for adequate blood flow, but also have a mechanism in place that helps to minimize bleeding when injury takes place. For our earliest ancestors, this would be the difference between life and death.
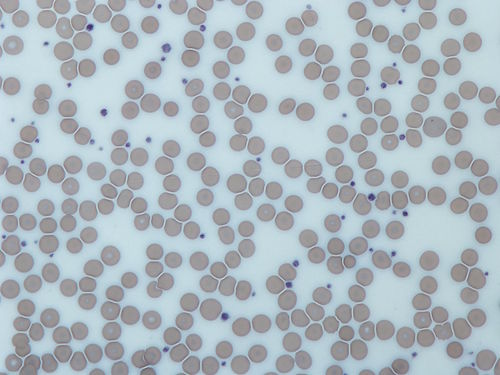
The second action needed for clot formation and hemostasis is the activation of the platelets. Platelets, also known as thrombocytes, are small disc-shaped, cell-like structures in the blood. They are about one-quarter to one-half the size of red blood cells. Platelets form in the bone marrow and, once released into the bloodstream, survive for only about ten days.
Platelet production in the bone marrow is controlled by a hormone called thrombopoietin. This hormone is produced mainly in the liver and the kidneys. It works by attaching to specific receptors on the stem cells in the bone marrow to start the production of platelets. How the body regulates thrombopoietin production has only recently been explored, and where the thrombopoietin receptor on the stem cells originated is still unknown. But rest assured, this lack of knowledge does not deter evolutionists from speculating on how platelets with their important function must have come into being only by chance and the laws of nature alone.
Normally, platelets circulate in the bloodstream without interacting with each other or the blood vessel wall. This occurs because the endothelium releases chemicals that prevent the platelets from sticking to each other and repels them from the vessel wall. Vascular injury activates the platelets by disrupting the secretion of these endothelial chemicals and exposes the platelets to the collagen just below the endothelium as well. This allows the platelets passing by the damaged region to attach to the vessel wall, change shape, and stick together.
Activated platelets also release chemicals that cause further vasconstriction and recruit more passing platelets to the site of injury. This piling on of several layers of platelets sticking to each other is called platelet aggregation, and it ultimately results in the formation of a soft platelet plug. Since the vessel walls on either side of the injury still have an intact endothelium, platelet activation and plug formation tends to be limited mainly to the site of injury. In this way, progression of the platelet plug in either direction from the vessel injury is usually prevented. The total absence of platelets is incompatible with life.
For minor injuries in very small blood vessels, the platelet plug is often all that is needed to stop the bleeding and allow healing to take place. Think of it like what a beaver must do to fix a breach in its dam. If it is very small with only a trickle of water going through, then using small amounts of soft leaves and sticks joined together by thin mud may be all that is needed. But if it is larger and has a torrent of water going through, then lots of large logs and flexible branches combined with solid sticks, soft leaves, and lots of thick mud will be needed to seal the breach.
For most of the traumatic injuries our earliest ancestors encountered in trying to win the battle for survival, it is the latter situation that applied. Next time, we’ll look at how the third component needed for adequate hemostasis, the clotting factors, bring about fibrin clot formation to prevent excessive blood loss.
Image: Platelets, shown as blue dots, and red blood cells, by Graham Beards, [GFDL or CC BY-SA 4.0-3.0-2.5-2.0-1.0], via Wikimedia Commons.
{kind=link}